Patients usually have a record of their medical history in hospitals or with medical practitioners as files or smartcards. These records are the main source of information that you and other doctors need to review a patient’s health. As such, the health history form becomes a critical document that you will ask new patients to fill out.
Table of Contents
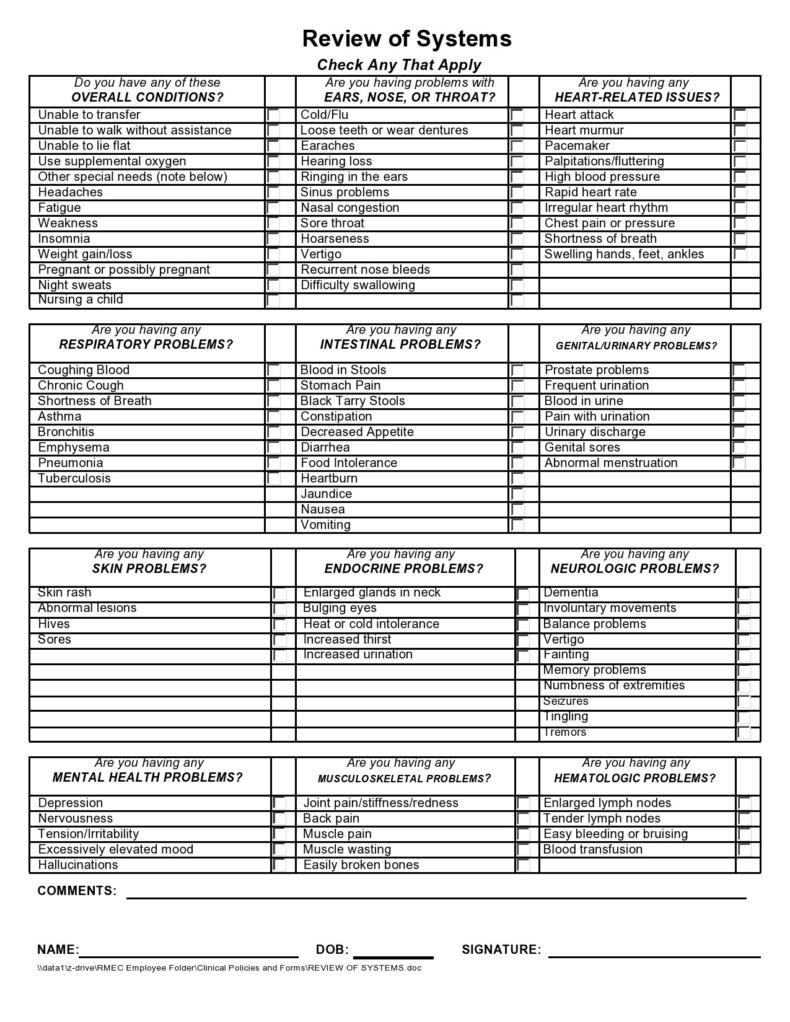
Health History Forms









What is a medical history form?
When patients fill up health history forms before their consultation, they might have wonder why it matters – whether their grandparents had diabetes, high blood pressure, or any other chronic disease as such. Your forms usually include routine questions like this.
A medical history form generally includes both a patient’s personal health history and their family’s health history. The first one provides details about the health issues a patient has had and the second one provides details about health problems that their blood relatives have had throughout their lives.
Taken together, this information provides you with important indications about what’s going on with a patient’s health because of the diseases that run in their family. Aside from this, you will also get to inform your patients what health problems they may be at risk for in the future.
Medical History Forms










What is the purpose of this form?
The patient medical history form is very important in a number of ways. For one, insurance firms use them as a basis for the insurability of a patient. But the main purpose of the form is to provide you with important information about a patient’s health history, risk factors, and care requirements.
There are various types of health history forms, each of which differs from the other. For instance, there are forms:
- That you use specific types of medicines.
- That therapists use, which have intensive and lengthy questions that focus on psychiatric concerns, and might include information like queries on anxiety, hearing voices, and so on.
- That you use for a patient’s history of mental disorders. For this, each member of the family must have a separate document.
Health History Questionnaires










What is a health history questionnaire?
When patients consult with you, it’s common practice to ask them are to fill in a health history questionnaire for medical purposes. This is a collection of organized information that’s unique to every person.
Relevant aspects of the health history form questionnaire usually include demographic, biographical, mental, physical, socio-cultural, emotional, spiritual, and sexual data. The medical history form can help you and your patients as it provides information that can assist with the diagnosis, the establishment of trust, and treatment decisions.
In addition, the information can also help in determining a patient’s baseline or what’s expected or normal for the person. As implemented today, each person must have a comprehensive health history documented as a part of their regular physical examination.
One of the most common methods for getting a person’s health history is through a clinical interview that involves asking health history questions. This can be an important means of securing information, especially if you can effectively communicate with your patients.
You can get the sources of information that comprise the health history from a patient’s previous records, the patient, their caretakers, or their significant others. The length and depth of the history-taking process depend on several factors like the patient’s purpose of the visit, the urgency of their condition or complaint, and so on.
Depending on the circumstances, history can be very comprehensive and holistic although sometimes, it’s only a brief review of the most relevant facts. In those instances where you shorten the history-gathering process, it will only focus on the patient’s medical experiences.
There are several ways to organize health histories. In many organizations, they typically provide a template, form, or computer database that serves as a documentation tool and guide for medical history. In general, the first part covered by history is data identification.
Questions to include
Most health history form questionnaires consist of a set of questions that will help guide you in understanding the population you provide medical services to. The questions in a patient medical history form are very helpful to medical researchers, medical clinics, and hospitals too.
The information gathered from these health history questions makes it easier for you to make an analysis or a diagnosis. In order for you to optimally treat your patient, you must know the details of their medical history. Here are some of the most important questions to include in a patient or family medical history form questionnaire:
- Demographic Questions
One of the most important aspects of a questionnaire is the questions related to demographics as these help you determine the factors that may influence the patient’s ability to make decisions. Here are some of the most common questions on demographics:
What’s your age?
What’s your ethnicity
What’s your highest educational level
What’s your marital status?
What’s your employment status - Health History Questions
Have you ever received treatment in an ER?
Were you ever rushed to the hospital in an ambulance? If yes, for what reason?
Have you ever had an allergic reaction? If yes, to what?
Do you carry medication in case of emergencies?
Do you wear a bracelet or any other medical jewelry?
Have you ever received stitches?
Were you ever admitted to the hospital? If yes, for what?
Have you ever experienced a sprain or fracture?
Were you ever denied medical insurance?
Family Medical History Forms














How do you create a health history?
Discovering a person’s health history can help them in two ways – first, to understand their past better and form meaningful connections with the members of their family. Many health conditions have something to do with heredity as these get passed down through generations.
Some of these health issues include high blood pressure, certain types of cancer, heart disease, diabetes, and many more. Making a health history questionnaire can be very useful in gathering and recording important medical information that can help:
- Recognize early signs and symptoms. Early diagnosis and treatment may lead to better outcomes.
- Request tests or screenings targeted toward people at high risk of developing certain conditions.
- You explain the importance of making lifestyle changes to lower a patient’s risks.
- Share a patient’s family medical information with you so that you can suggest other ways to keep them healthy or improve their treatment.
A person’s medical history form is continuously updated through the years and these updates are usually the information added after every visit with you. Here are some steps to create a health history with relevant health history questions:
- Instruct your patient to speak with the members of their family
Conversations regarding health and medical issues can often make people feel uncomfortable because the information is both private and sensitive. If a patient has to talk about these with their family members, they can do this in a place that’s private.
Explain to them why you need to know about their health and advise your patient to ask their family member’s permission since they will share the information outside of the family.
Only ask for relevant information and only if truly necessary. The information you gather can be very helpful, especially if you’re not familiar with the patient’s racial heritage because there are some conditions and diseases that manifest themselves in specific races. - Obtain other information from your patient’s previous records
Talking to family members will not be sufficient in learning more about a patient’s health. This is because family members may feel reluctant to share or maybe the information isn’t widely known. Aside from asking your patient to talk to their family members, you can also check their previous records to collect more data about the patient’s family history.
You can even go as far as checking death records as these often include a cause of death. Many early death records leave the cause of death blank, they record these as “unknown,” or they describe these with non-specific phrases like “old age” or “childhood disease.”
Other records might list diseases that aren’t familiar because people then used different terminologies. A little research can help you solve the mystery for these outdated terminologies. Other sources about your patient’s health can include medical records, funeral home records, and obituaries. - Document everything you discover
Make it a point to record all the medical and health information you have gathered about your patient. This compilation can reveal important patterns about diseases in their family. Additionally, it becomes much easier for you to readily share the information.
After you have compiled the information about your patient’s health history, don’t forget to include everything you have learned from such. You can write this important health information in a separate document so that others could access it too. Just remember that you should never share or disclose information for people who are still alive. - Share the results
Heredity usually involves family and as such, each family member might also be at risk for the same conditions that your patient suffers from. It is important to share what you have uncovered with your patient’s family members so they can also benefit from the research you have done.
Of course, you must also inform your patient about what you have learned. If you made a report about their health history, you can give a copy to them.