People who go to the hospital seeking medical information or help will be first attended by any member of the nursing staff before going to a doctor. As a nurse, you would perform a nursing assessment, which includes height and weight measurements, temperature, blood pressure, heart, and respiratory rate. You record your results in a nursing assessment form.
Table of Contents
Nursing Assessment Forms










What is a nursing assessment?
A nursing assessment form contains a collection of information about the physiological, psychological, spiritual, and sociological status of a patient. The assessment is the first step in the nursing process.
Although you can use nursing skin assessment forms and other forms to identify the current and future needs of a patient, it still has a very broad scope. You should go through certain set procedures before you can properly evaluate an individual.
Typically, you will use a nursing assessment sheet that you will fill up when conducting these evaluations. The nursing assessment is an organized set of processes you use to provide optimal care for your patients.
You cannot delegate this assessment to unlicensed nurses, although nursing students unless with the guidance of their clinical instructors. This assessment has a broad scope because it focuses on the whole body system. There are different types that focus only on specific parts of the assessment. These include:
- Learning Needs
Here, you identify deficiencies in knowledge that serve as the basis of the learning needs of a person that you can analyze. This functions as a guide in teaching by a healthcare provider. - Competency
This is the continuous evaluation of the knowledge, skills, and development of a person that enables them to perform activities. - Physical
This is a thorough head-to-toe assessment of a patient. - Admission
Before a patient gets confined in a hospital, they must go through physical assessments and statistics. This serves as a baseline for the required actions you must take and for the patient records. - Holistic
This approach toward a patient involves sociological, cultural, spiritual, and psychological needs. You derive your nursing implementations from the information you gather from your patient.
Nursing Assessment Templates










Why is a nursing assessment important?
In general, nurses know that a comprehensive nursing assessment is an important first step in the development of a plan to deliver the best possible patient care. As a nurse, you also know that a nursing assessment form is a key part of your responsibilities and roles.
A nursing assessment example is a tool used to learn about a patient’s symptoms, overall health, and concerns. A nursing assessment template is an essential factor because this is where you gather comprehensive data to help in the determination of your diagnoses, which you then use to develop nursing care plans to help improve health outcomes.
The comprehensive data on these forms include psychological, socioeconomic, social, and physiological determinants of health, lifestyle, and spiritual information. The comprehensive health assessment has many components.
Before the assessment begins, you must develop a rapport with your patients by first introducing yourself, then explaining what you will do during the assessment and why.
Patients become anxious when you conduct these assessments and establishing a rapport with them helps put them at ease although this could also depend upon the setting of the assessment or the reason for their visit.
Most comprehensive nursing assessments usually begin with the health history of the patient and this includes information about their past injuries or illnesses including childhood immunizations and illnesses, surgeries, hospitalizations, allergies, chronic illnesses, and the illnesses that run in their family.
One of the components of a nursing assessment is the health history of the patient. Here, you will ask a patient to describe the symptoms they feel, when their symptoms began, and how they developed before you forward the process to the physical examination.
Physical examinations are very familiar to most people and they usually start with a complete set of vital signs including blood pressure, respiratory rate, temperature, and heart rate.
Because of the increasing rate of chronic conditions and the growing elderly population, it is necessary to learn how to keep up with distinct patient characteristics. This is another important aspect of the BSN and RN program.
Nursing Assessment Examples










How do you write a nursing assessment?
One of the most important roles of filling out nursing assessment examples is to provide accurate, safe, and effective nursing care. This is the first step in the nursing process and it involves exploring the psychological, physical, social, and spiritual aspects of a patient.
In other words, nursing skin assessment forms and other forms are a systematic and holistic guide for you to gain a better understanding of the needs and wants of a patient. A nursing assessment sheet is the underlying foundation of the process on which you base the other parts of the process.
You use the nursing assessment form as the starting point to building a therapeutic patient-nurse relationship and you can establish this during your first encounter. Actually, the assessment is the first encounter between you and a patient. You will both make first impressions and these judgments can have a great effect on how a patient perceives you.
Through this assessment, you can get information essential for providing your patient with effective holistic care. You can use nursing assessment framework tools to get from a patient, accurate information about them.
The initial assessment, which you based on both objective and subjective data, can be your basis in determining the actual issues of a patient, as well as, any potential issues. When making this assessment, include the following:
- Admission Assessment
You should complete this with the patient, a caregiver, or a parent upon the patient’s arrival and you must be complete it within 24 hours of their admission. Then you enter any additional information into the progress notes of the patient. It is important to consider the privacy of your patient at all times. - Patient History
As a nurse, you should discuss the following with your patient:
The history of the patient’s current injury or illness
Other relevant details about their past history
Any allergies and similar reactions
Any medications the patient is currently taking
Immunization status
Implants, social, and family history
You should also discuss any recent overseas travel and documented this information
Assessment of your patients’ overall emotional, behavioral, and physical state. You should conduct this upon their admission then continue to observe them throughout their stay in the hospital. - Vital Signs
This involves recording baseline observations on your patient’s observation flowsheet. This is an important aspect of admission documentation and assessment. You should complete an ongoing assessment of vital signs as indicated for your patient.
It is very important to review the VICTOR graph every two hours or as your patient’s condition requires. This allows you to observe any trending of vital signs that might support your clinical assessment process. - Physical Assessment
Conducting a structured physical examination can help you get a complete assessment of your patient. Some techniques used to obtain this information include inspection or observation, percussion, auscultation, and palpation. You should use your clinical judgment to decide on the extent of the assessment needed. Assessment information includes, but isn’t limited to:
Primary assessment
Shift Assessment
Focused Assessment
Neurological System
A complete neurological nursing assessment includes sensory function, neurological observations, growth and development including gross and fine motor skills.
seizures and other concerns.
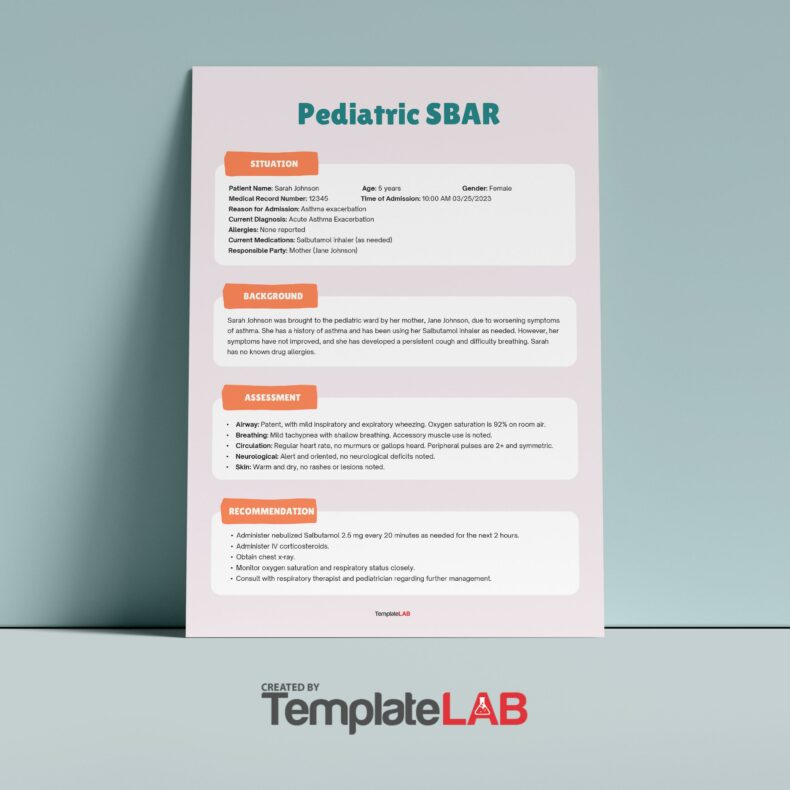
Respiratory System
Generally, children are more susceptible to respiratory illnesses and other similar conditions that cause respiratory distress. Therefore, you should conduct an assessment of the severity of their respiratory conditions.
Gastrointestinal
Ensure that your patient’s stomach isn’t full when conducting this assessment as this might induce vomiting. This assessment can include inspection, light palpation and auscultation of the abdomen to find visible abnormalities, softness or tenderness and bowel sounds.
Musculoskeletal
You can conduct this assessment while observing a child or in bed or as they move about a room. Keep in mind that during periods of rapid growth, children usually complain of normal muscle aches. You should compare their joints and limbs bilaterally throughout your assessment.
Skin
You conduct this to identify any cutaneous issues or systematic diseases.
Eye
You should perform eye inspection on children very carefully and only when the child is completely compliant.
Ear, Nose, and Throat (ENT)
Conducting this assessment is important as respiratory illnesses are very common in children. It should also involve a comprehensive examination of the throat, the mouth, and the oral cavity. Common diseases here might include allergies, upper respiratory infections, facial or oral trauma, pharyngitis and dental caries. - Assessment Evaluation
Make sure that the information you collect is properly documented, complete, and accurate before going to the evaluation phase of your assessment. You must use problem-solving and critical thinking skills in making clinical decisions and the plan of care for the patient you’re assessing.
Should you discover any abnormal findings, it will be your responsibility to take appropriate action. These actions may include communicating your findings to the medical team, the ANUM in charge of your shift, or related allied health team. Patients should undergo continuous assessment for any changes in their condition while under your care. Moreover, these assessments should be regularly documented.
Nursing Assessment Sheets