When used in medical settings, the “DAP” in DAP notes stands for “Diagnostic Assessment Program.” When you use DAP note examples in healthcare institutions, you would follow the standard format that includes data, assessment, response, and a plan for the medical care of your patients. In DAP progress notes, you would also include the contact information of your patient, the summary and assessment of your patient’s problem, and the treatment plan.
Table of Contents
DAP Notes









What is a DAP note?
DAP notes are a type of documentation method used by social workers, healthcare providers, and other medical professionals. The format used for a DAP note template is ideal when keeping track of the behavioral health of patients.
What goes in a DAP note?
The main goal of a DAP note example is to ensure that you take consider all of the objective and subjective information for the immediate care of your patient. It also includes an assessment that you base on the condition of your patient balanced from your objective and subjective analyses.
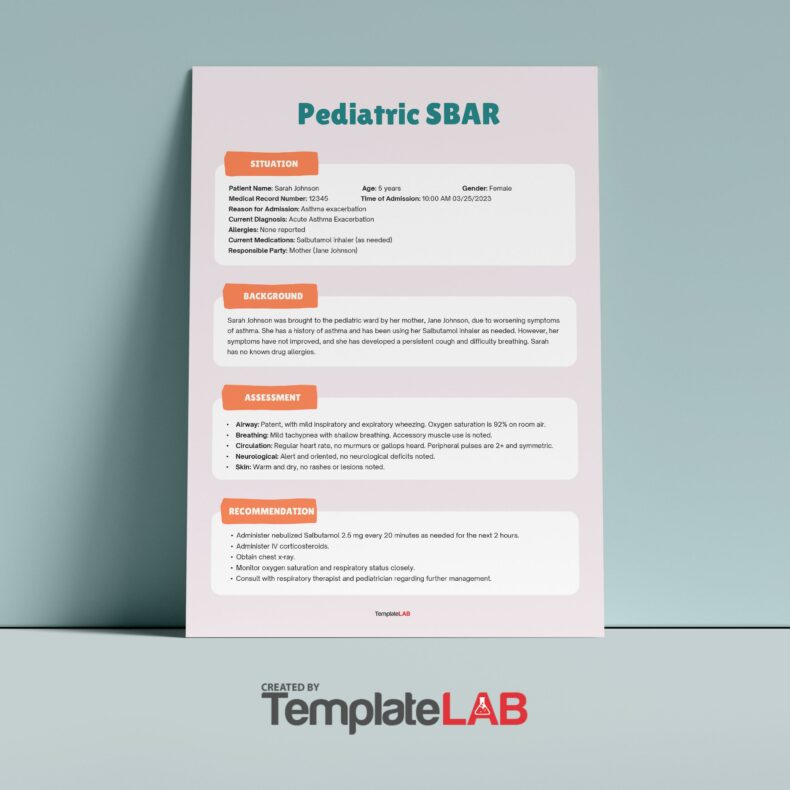
DAP is a standard documentation method. This means that you can’t just write anything you want in DAP notes. Here are the basic information to include when creating your patient’s DAP progress notes:
- Subjective observation
The basis of this data is what your patient feels about his/her condition along with your patient’s thoughts and observations about his/her condition too. The aim of subjective observation is to determine the nature of your patient’s pain based on how he/she describes it. - Objective observation
The basis of this data is what you (or the healthcare provider) observes about the condition of your patient. Including this information helps list, narrow down, and isolate your patient’s likeliest condition.
Make sure to write down all of the observable visual data like circulation, palpitation, neurological, and visual assessment. You may also include observations about your patient’s appearance and mood. - Assessment
Here, you write down your understanding of your patient’s problem and provide a working hypothesis. Include here the most probable diagnosis of your patient’s condition since you don’t have a conclusive diagnosis yet.
In this part of a DAP note template, you may also include the results of all screening tests your patient had undergone along with a referral to a specialist if any. Here, you may also include the type of condition whether it’s recurring, acute or chronic. - Plan
For this part, write down the necessary steps for the treatment of your patient. The type of treatment may include therapy, medications, surgery, and more depending on your patient’s condition. Set the short-term and long-term treatment and any lifestyle changes your patient needs to make.
The main aim of the plan is to reduce the pain felt by your patient and help them heal. Depending on how your patient responds to the treatment, you may also include any revisions that you consider including how many sessions he/she needs and the dates of these sessions.
Apart from all of this basic information, you should also check your patient’s personal name, identifier, and if all handwriting has been legibly done. This is important so that other healthcare providers can use DAP notes to treat your patients. Finally, make sure that you sign the note and date it to make it valid.
DAP Note Examples










Tips for creating your DAP notes
Creating an effective DAP note example for therapy sessions doesn’t have to be a challenge. Using a DAP note template is the best method of taking notes in an effective, quick, and useful way. To help you create these notes, here are some tips:
- Define what the perfect note is
When you write notes, try to imagine what the perfect note is for you. While you can’t write a “perfect DAP note,” you should at least have a good understanding of the outcome you want. This helps you work towards it. After making the choice to use this method, make sure to customize the information on it to suit your needs.
For this, you may have to ask yourself a few questions including:
What information do you need about your patient so that you can create a good treatment plan?
If another healthcare professional would write the DAP progress notes, what information would you find helpful or usable?
After answering these questions, you can start thinking about how each part of your notes would look like. For this, you need to make sure to present all sections in a quick and effective way. - Keep things simple
While writing your notes, you should get as much valuable information from your patient as possible – just don’t overcomplicate things. Familiarize yourself with the type of information you want to include and the type of information you don’t want to include in your notes. The point here is to avoid writing too many descriptions or explanations while still maintaining thoroughness and usefulness. - Use the tools that best suit your needs
One thing you need to consider when writing your notes is what you plan to use for taking down notes. You can either use a DAP template online right away or write your notes down on paper then type them online when you get the chance.
If you’re not sure which method to use, you may start by using templates first. This gives you a chance to ensure that you’re recording all of the information you need at each session. Try switching between methods to see which one works best for you.
Writing DAP notes using the proper format
When writing progress notes in DAP, follow the standard organizational format. When writing clinical progress notes, include your patient’s contact information, the summary and assessment of your patient’s problem, and any treatment plans. Take down your notes by hand or use your computer. Do whatever’s easier for you then use these tips to follow the proper format:
- Write your notes in the data section
This is the most important section of your notes and it is where you include your patient’s contact information, objective and subjective data, and any observational notes you have from the most recent session.
The objective data consists of the information you observe while interacting with your patient like facial expressions, body movements, and more. The subjective data consists of a summary of information provided by your patient. You may even include quotes from your patient. - Write your notes in the assessment/response section
This section contains the summary of your professional opinions and ideas based on the objective and subjective information you’ve gathered. Here, include your ideas, thoughts, feeling, and the rationale for your ideas. You may also include observations about the progress you perceive in your patient. - Write your notes in the plan section
Write down the treatment plan you have decided on in this section. Take note of any changes you make in your treatment plan depending on the sessions you have with your patient. Also, include any thoughts of work you still need to do in your next sessions along with notes about interventions or referrals that you have completed or that you recommend.
DAP Note Templates









Mistakes to avoid when writing DAP notes
DAP notes should indicate that you provided quality care to your patient while respecting his/her wishes and condition. While writing these notes, here are some mistakes to avoid to ensure effectiveness:
- Don’t make your notes too long
Write down all of the important information you need without adding unnecessary details. Don’t exclude any information, especially when you think it’s critical for the explanation of treatment plans. - Don’t forget to write your notes clearly
Remember that other healthcare professionals may have to read your notes. Therefore, you should write as legibly as possible to ensure that they can understand everything and help your patient without delay. - Don’t violate your patient’s privacy
While writing your notes, keep your patient’s privacy in mind. For instance, don’t quote or name anyone that your patient mentions during your sessions. Also, if your patient shares any sensitive information about himself/herself, don’t include this in your notes. - Don’t include complaints about other staff members, whether from the patient, staff, or a doctor
Even if your patient complains about any other patient, staff member, doctor or anyone else he/she has interacted with, you shouldn’t include those comments here. For instance, if your patient had a bad experience with one of the doctors you recommended him/her to, they may complain about it to you.
This is an example of information that you shouldn’t include in your notes. After all, it doesn’t directly affect your patient’s condition. The more you practice determining what information is necessary and what information isn’t, the easier it becomes for you.
Never include names in your notes no matter how frequently your patient repeats them. Instead, use terms like patient, doctor, staff member, and so on. That way you can still include pertinent details without giving out any specifics. - Don’t ever include any pejorative or derogatory statements about your patient
As a healthcare professional, you should always convey respect and concern for your patient no matter what his/her condition is. If you feel like you cannot remain professional with your patient, recommend or refer him/her to another doctor.